
by Leif Kullman
This month we are going to look at a couple of patients. It must be emphasised, that it is seldom possible to state a definitive diagnosis based upon the roentgenological appearance.
A strict clinical investigation before the radiographs are taken, is a must, it will control that the correct radiographic investigation is performed. And of course it is also important to have relevant anamnestic records.
The first patient is a 9 year old girl, arriving as an emergency dental patient to the clinic since she and her parents have noticed a progressive swelling in her right side during a long time. The patient has not had any pain or other subjective symptoms from the region.
When a panoramic radiograph is taken (fig.1) the following image is seen:

Figure 1.
Some additional radiographs are taken and we write in our statement
The panoramic (OPG) film reveals a radiolucent area within the right body of mandible, with extension and expansion of the lesion up into the right ramus.
The developing 48 has been superiorly displaced towards the region of the coronoid process and marked expansion of the inferior and facial bony cortex is revealed in a frontal view, which also was taken. The lesion is predominately well circumscribed with a tendency to mutilocularity. There appear to be small septa-like features contained within this area of radiolucency. There is thinning of the cortex in several parts of the peripheral extensions of the lesion. Some root resorption of particularly 47 is noted.
Possible differential diagnosis to consider according to this description are different odontogenic cysts or tumors, an aneurysmal bone cyst or central giant cell lesion or central myxoma. There are more that can be considered- among other things central haemangiomas, fibromas and also neurogenic tumors and cherubism. Perhaps the most likely of all these is an dentigerous cyst.
An operation was performed and the pathology report was that it was an aneurysmal bone cyst. During the follow up period, no fast healing have been seen, but on the contrary- the lesion seems mainly unchanged and a reoperation is today considered. It cannot be excluded that a new diagnosis will be stated after this.
The next patient is a female about 60 years old. She has noticed a minor swelling
occasionally the last 6 months in the left mandibular angle area and inthe cheek and has felt a thudding feeling in the same area. Her permanent dentist makes an investigation but cannot find any explanation and the patient visits a ear, nose and throat specialist to get further help.
A panoramic radiograph is taken of the jaws and the nose and throat specialist diagnose a radiopaque area in connection to the apex of the tooth 34 (arrow in fig. 2).

Figure 2.
The diagnosis salivary calculus of the submaxillary duct is stated and the patient gets a new appointment time for a removal of this.
However, the day that this operation should take place, the doctor still had some doubts about the diagnosis and therefore sent the patient to our radiology department for a supplementary examination.

Figure 3.
We take an occlusal view of the floor of the mouth (fig. 3) and find no signs of a salivary calculus and in an introral radiograph against the periapical region of 34 the radiopacity can be seen in the same place as in the panoramic radiograph (fig. 4).
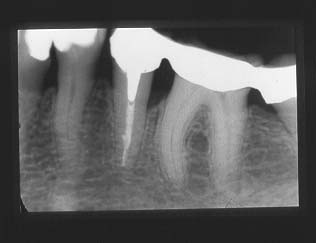
Figure 4.
Our suggestion to a diagnosis became now condensing osteitis 34 and this can be verified when a root canal treatment id started the same day (fig. 5).
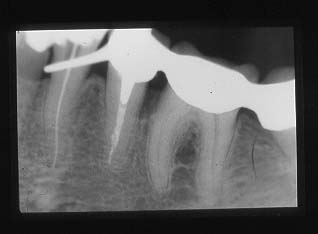
Figure 5.
Next month my friend and colleague in Australia, Ross McDonald will tell us some interesting matters from the southern hemisphere.
Leif Kullman