
by Leif Kullman
The temporomandibular joint (TMJ).
I will this month report about some useful radiographic
methods to investigate the temporomandibular joint and I will also make a case
description.
The temporomandibular joint is, as well as the whole dentomaxillofacial region, of a complex anatomy. However radiography is an important and accurate investigation method to assist the klinician in establishing differential diagnosis of different pathology in the TMz.
|PTraditionally different plain`radiographic methods have been used, using multidirectional projections, such as transcranial and transpharyngeal`to be able to visualize the components of the TMJ as good as possible. However only larger pathological changes can be seen well in plain radiographs of the TMJ qnd the same drawback is valid for our modern panoramic examinations.`Therefore, during the last decades, different tomographic radiological methods have wrown popular. It has for example been shown that hypocycloidal tomography in a sagittal and vrontal projection is accurate to detect small structural changes in the bone. Different slice thickness can be used. The most common method is probably a tomographic view, where the &127;sseous structures of the mandibular condyle and fossa are seen from a lateral projection. The internal position of the bony structures of the TMJ when the teeth are in occlusion and during mouth opening can be studied.
Today we know that the major problem for many patients is not only the osseous structures but rather damages to the articular disc and its attachment ligaments and the capsular tissue. These patients suffer from a`so called internal derangement. In these cases the above mentioned methods are not enough, since they don't visualize the soft tissue of the TMJ. To get rid of this shortcoming, a radiopaque contrast solution can be injected into the joint before the examination, we can perform an arthrographic examination, where also a hypocycloidal tomographic method for example is used. However even this method has drawbacks, it is for example an invasive radiographic examination, which needs sterile surrounding procedures and local anesthesia. During the last decade two other methods have therefore grown popular as imaging tool for the TMJ, CT (computed tomography) and MRI (Magnetic Resonance Imaging). It can be read more about these methods in i.e. my monthly messages from April and September 1997.
CT has its strength in its ability to produce slices with a high quality of the bony structures of the joint but has also been used for evaluation of the soft tissues. However the contrast for soft tissue imaging is more perfect in MRI examinations and this method is therefore most useful for the TMJ. As a matter of fact it is the only imaging technique that visualize both the soft tissues and the osseous structures of the TMJ including the disk with its posterior attachment very well.
A case
Everything started with a hamburger meal: I mean the symptom. My daughter, one day
experienced problem to open her mouth full to take a big bite from her hamburger.
She felt pain when she opened up maximum and could hear sounds from her TMJ¥s during this. The sound was on the left side and it was distinct and reciprocal being heard during the opening and closing of the mouth. In the other side there was some pain, but no sound. We arranged with an appointment to a specialist in TMJ and my daughter obtained a splint to use particular during the nights.
Nothing dramatically happened for a couple of years. My daughter had continuous minor TMJ problem, as the described above. Perhaps she was not the most perfect patient. Sometimes she neglected her prescription partly depending on that the symptoms were very small, almost not existing some days.
With a father, working as a radiologist, we decided to make a tomographic examination. A preliminary panoramic overview showed no certain pathology, but minor suspected hard tissue changes in both sides could be suspected (figure 1)

Since we had a hypocycloidal equipment at my working place, we also performed an investigation with this. In figure 2 one image from this occasion can be seen. In this image some osseous structural changes could be seen including a flattening of the condyle in the right side.
 Figure 2.
Figure 2.
Since we suspected an internal derangement, based upon the clinical findings and subjective symptoms we followed up these examinations with a MRI-investigation. The images from this (see one of them in figure 3) confirmed the diagnosis that we had suspected: An ADD without reduction in the right side (anteriorly displaced disk) and with reduction in the left side.
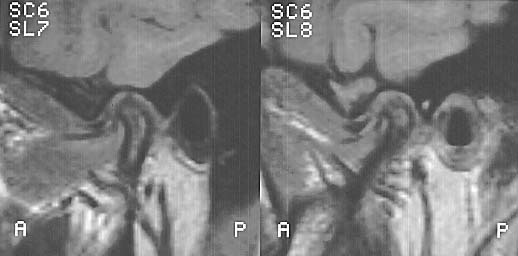
Figure 3.
Next month I will do like most other people in Sweden. Take holidays from my usual work and my ODIS writing. But in August I will be back again and report a little about radiology in implant therapy.